
Depression is a common thread among all humans – this isn’t limited to MTHFR folks in any way, but as folks with an MTHFR variant, balancing methylation can be an effective way of tackling depression that is often overlooked by doctors and practitioners.
We always hear about neurotransmitters and depression, so much so, that I feel we overlook the fact that there are any other possible contributors. The assumption becomes that if you’re depressed, your neurotransmitters must be off somehow and if we can fix those neurotransmitters, we can fix the depression.
The problem is, this theory doesn’t actually pan out for a lot of people – especially MTHFR people. A drug that boosts the activity of serotonin in the brain should work, but often doesn’t. It has a lot of merit to explore other cuases of depression as well – especially when so many of them are fixable.
MTHFR does, of course, affect neurotransmitters via the BH4 pathway, but my experience clinically has been that balancing all of the other things goes farther than pills for neurotransmitters in most people (there are some highly notable exceptions, of course.)
Many factors play into depression and some of these are related to MTHFR, and some aren’t.
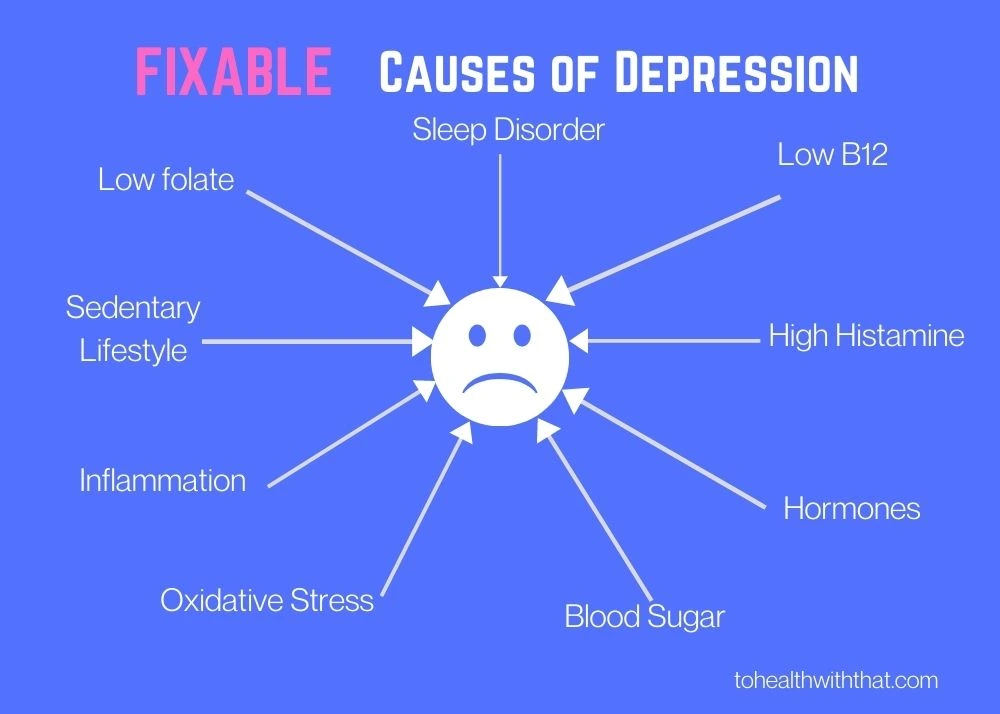
- Low Folate and Vitamin B12 Status – This link holds true whether the person in question has an MTHFR issue or not. Lower nutritional status regarding folate and B12 means a higher risk of depression. Also, higher serum B12 and folate are shown to predict better treatment outcomes.
- MTHFR? – It is clear that lower folate levels can increase the risk of depression, and that MTHFR can increase the risk of lower folate levels, but it isn’t absolutely clear if MTHFR increases the risk of depression independently from folate status. There are several ways that it could – MTHFR polymorphisms have an impact on neurotransmitter formation, and also on DNA methylation, which can boost depression by itself.
- C677T Status? – Again, this is questionable. This meta-analysis shows a link between C677T status and depression, but the fascinating thing is that another study shows that the strength of the link changes in different geographical areas. This could be due to local changes in diet, but it could also represent a big wild-card factor that tells us we have a lot to learn in this area.
- High homocysteine – Of course high homocysteine could be a result of low folate status, but there is a clear link between homocysteine and depression (and, don’t forget, a link between MTHFR and homocysteine.)
- Inflammation – In a classic chicken-or-egg scenario, inflammation and depression are terminally linked. If inflammation rises, so too does depression and likewise, if depression worsens, so too does inflammation. With MTHFR we do have a greater tendency toward both, so it matters to keep your inflammatory processes in check.
- Oxidative stress – Oxidative stress is your body’s total level of reactive oxygen species (free radicals). Studies show that people with higher levels of markers for oxidative stress also have higher levels of depression and poorer responses to treatment. With MTHFR, we have the potential to have lower glutathione, which is the master antioxidant, meaning we may have higher levels of oxidative stress.
- Insulin Resistance and Blood Sugar Issues – Research is mixed in this area. There is a clear link between depression and diabetes, but insulin resistance, which is one of the stepping stones on the path to type 2 diabetes, is less clear. The immediate and obvious link between blood sugar fluctuations and mood, is much less difficult. As anyone with a hungry toddler can tell you, the jump between hungry and “hangry” is a short one. Again, with MTHFR we do have a slightly increased tendency towards blood sugar issues, insulin resistance, and ultimately diabetes.
- Hormones – Again, the links here aren’t clear. Low estrogen in women is linked to perimenopausal depression. Low Testosterone in men is likewise linked to depression. High estrogen presents mood and behavior shifts, and high progesterone brings on the waterworks (between naps). What is clear is that balanced hormones certainly lead to better and steadier moods, where fluctuations or abnormalities might put us into the roughs. MTHFR is, of course, involved in hormone regulation and processing, so righting the balance can be a highly productive step.
- Sleep – A giant link exists between sleep quality and depression, and most of us have firsthand experience of that (is anybody else’s household entirely grumpy if their sleep is interrupted?)
- Sedentary Lifestyle – There isn’t particularly a link between MTHFR and sedentary lifestyles, which is great news. There is, however, a big link between sedentary behavior and depression and also between exercise and improved quality of life mentally, emotionally, and physically. This isn’t an MTHFR issue in any way, but I would feel remiss if I left it out of the causes of depression list.
Each of the factors above is measurable and trackable and highly treatable, with or without an MTHFR mutation. Each of those factors can be worked on independently, but also any step toward a healthier lifestyle is going to help in many of those areas.
For example, balancing your methylation (which for us MTHFR folks usually means either taking a good form of folate or if we don’t tolerate folate, then finding a good work-around) will help to raise folate levels, lower homocysteine, and reduce both inflammation and oxidative stress. So one change is influencing four big contributing factors to depression. Does that mean balancing your methylation is going to fix your depression completely? Not necessarily, but it does get us closer to the goal and also improve your chances of responding better to other therapeutic interventions as well.
So from this list, we have a number of natural treatments for depression:
- Folate, high folate diet, and anything that will help you to balance your methylation
- B12
- Exercise
- Any kind of sleep therapy
- Lower glycemic index diet for blood sugars
- Reducing inflammatory foods
- Antioxidants – especially the ones that cross the blood-brain barrier
- Anything that will help you balance your hormones
- Any anti-inflammatory

Every one of those is a book in and of itself, but seriously that is a lot of options to try, and all of them will lead to greater health regardless.
There are also two special factors that we haven’t talked about yet. One pertains more strongly to MTHFR folks, and the other is just a human-nature problem.
- Childhood Trauma – A significant portion of depression in adults stems from childhood trauma, and unfortunately, people with the MTHFR mutations may be more susceptible to life-long depressive tendencies from childhood traumas than average. This is fixable, but it will take some work. This could be self-guided help through spiritual seeking, prayer, meditation, and self-healing techniques. It could also be professional help in the form of therapy, hypnosis, EMDR, or a myriad of other options.
- Habit – This conversation is really neglected and so next week’s topic is going to be about expanding the habit idea and giving you some life hacks that you can start to practice at home, but any mental state, no matter what else contributes to it, has the potential for a habit component. This could be depression, anxiety, obsessive thoughts, intrusive thoughts, whatever. And sometimes you have to train yourself to break the habit in the same way that you would with any other bad habit.
I feel like all of this could appear daunting, but if you look at it another way, it also opens up so many opportunities for healing that are often overlooked. It can be incredibly discouraging when your doctor runs out of options for depression, but chances are they haven’t even scratched the surface of this list. Typically doctors look at sleep, blood sugar, and neurotransmitters in terms of depression. You now have the opportunity to dive deeper.
MTHFR is a common genetic mutation that can contribute to anxiety, depression, fatigue, chronic pain, infertility, and more serious conditions like breast implant illness, heart attack, stroke, chronic fatigue syndrome, and some types of cancer. If you know or suspect you have an MTHFR variant, schedule a free 15-minute meet-and-greet appointment with MTHFR expert Dr. Amy today.
Book Your Appointment

thank you for your dedication to being an amazing resource for health information. my wife has been on ssri’s 15 yrs for drug resistant depression/anxiety. do you have any significant position results in treating such extremely difficult cases? she is
62yrs, 120lbs, 5’7″, i introduced liver two weeks ago into our low carb/sugar diet but it seemed to make her anxiety become worse. I plan to try methlyated b complex in low does next week along with d3 and k. we eliminated folic acid. god bless. she can not sleep without prescribed narcotics.
Hi Don, I replied to your email as well, but here’s a public reply for everyone.
Your wife’s case sounds extremely challenging.
First off, if the liver seems to be causing more anxiety, try taking it back out of her diet and giving her a rest to let her symptoms calm down, then reintroducing smaller amounts slowly to see if she’ll tolerate any.
Be carefully about the methylated B complex, because if the folate in liver is enough to cause some anxiety, she might not be ready for a big jump to methylated Bs. The D3 and K shouldn’t be a problem, but the methylated Bs might.
Not being able to sleep is so difficult.
Always be careful with changes and move slowly. It sounds like your wife is very sensitive and it’s important not to overwhelm her system.